Using the Inflation Reduction Act to Rein in Pharmaceutical Company Abuses
The Case of Enbrel
By Jishian Ravinthiran & Steve Knievel
Key Findings
The Center for Medicare and Medicaid Services (CMS) and pharmaceutical manufacturers have now entered into agreements to negotiate prices of the first ten prescription drugs selected for Medicare drug price negotiations. These medicines treat an array of conditions, including heart failure, cancer, diabetes, and autoimmune diseases. [1] As CMS negotiates maximum fair prices for these drugs, it must consider how pharmaceutical industry abuses have artificially prolonged their monopolies, resulting in inflated prices, and use the full authority of the law to deliver just prices to its enrollees. This Report highlights the importance of accounting for unfair monopoly-extending practices in price negotiations by focusing on the selected drug etanercept (sold under the brand name Enbrel) which treats autoimmune diseases like rheumatoid arthritis.
- Medicare could have saved $1,053,023,122 in less than four years on just this one drug if biosimilar competitors had been allowed to enter the market when the underlying patent protection was set to expire in 2019.
- By the time maximum fair prices go into effect, Medicare will have lost nearly $ 2 billion ($1,891,500,836) because of unwarranted exclusivities protecting Enbrel from competition.
- Amgen, Enbrel’s manufacturer, gamed the patent system to deprive the public, Medicare, and its enrollees of more affordable alternatives. Amgen reworked old patent applications from another company to cover Enbrel once Amgen’s patent protection in the drug expired in 2019, so it could protect its monopoly power until 2029.
- Ignoring industry abuses that have resulted in inflated prices, as in Enbrel’s case, would detract from CMS’s mandate to deliver the lowest possible fair prices for Medicare’s enrollees. Where a manufacturer has gamed the patent system to unfairly extend exclusive control of a selected drug, CMS should consider (1) the prices that would be in place if proper competition existed, and (2) excessive revenues manufacturers have unfairly obtained from Medicare and its enrollees through this gamesmanship.
- In negotiating maximum fair prices for the selected drugs, CMS should not consider the facial value of acquisitions in research and development costs for a drug. In Enbrel’s case, Amgen acquired control of the drug by buying out a smaller company that originally manufactured it. The price tag of the acquisition, however, bears no relationship to the research and development costs of Enbrel that could help determine a fair price for the drug. Instead, these acquisition costs reflect the projected value of securing monopoly power to price drugs with minimal constraints. CMS should not allow companies to pass on those artificial costs to Medicare’s enrollees and taxpayers during the negotiations process.
Introduction
The passage of the Inflation Reduction Act (IRA) provides a powerful opportunity for the federal government to restore fairness to Medicare and its enrollees in accessing and using essential medicines. For the first time in its nearly 20-year history, Medicare can negotiate prices with pharmaceutical companies for selected drugs, instead of being forced to swallow the industry’s excessively high prices.[2]
From June 2022 to May 2023, Medicare Part D spent almost $3 billion dollars covering the prescription costs for Enbrel, a drug that treats autoimmune diseases, like rheumatoid arthritis, which disproportionately affect women.[3] That works out to about $60,000 per year for each Medicare enrollee prescribed the treatment, with an average out-of-pocket cost of more than $2,000 per year for just this drug among Part D patients who are non-low-income subsidy enrollees.[4]
Thanks to landmark provisions within the IRA, passed by congressional Democrats and signed into law by President Biden, Medicare will be able to negotiate a maximum fair price for selected drugs, including Enbrel, with significant cost savings to enrollees.[5] Amgen, the manufacturer of Enbrel, released a statement in light of the law’s passage arguing that “government price setting within Medicare will have a chilling effect on innovation at precisely the time when our nation needs more new medicines to treat an aging population.”[6]
Amgen, and industry more generally, would have us believe that the IRA’s negotiation scheme will detract from the ability to innovate new drugs, but that claim cannot be further from the truth. For example, a drug pricing investigation conducted by the House Oversight & Reform Committee found that Amgen spent far more on stock buybacks, dividends, and executive compensation than it did on research and development from 2016 through 2020.[7]
Amgen itself did not contribute to the research and development of Enbrel when it was first approved in 1998. In 2002, Amgen bought out the smaller company, Immunex, which originally manufactured the drug, for $16 billion to secure the lucrative potential of Enbrel. [8] While Amgen asserts that the IRA’s negotiation scheme will hurt innovation and access to medicines, it did nothing to contribute to the research and development of Enbrel before its approval in 1998.
After the acquisition, Amgen then deployed abusive patent practices to extend exclusivity of the drug for nearly three decades, far longer than the intellectual property protection typically afforded to medicines.[9] In doing so, Amgen prevented more affordable biosimilars from being used by Medicare and its enrollees.
The IRA’s negotiation provisions finally deliver to the government a powerful tool to curb the abuses of the pharmaceutical industry. But its success in delivering taxpayers and consumers relief from excessive pricing by drug corporations demands fully recognizing the pricing impacts of inappropriate monopoly extensions – starting with Enbrel. Enbrel’s history shows that inappropriate monopoly extensions through patent gamesmanship must be stressed in the evaluation by the drug price negotiation group of how manufacturer-submitted data impacts the maximum fair price. The Biden Administration should weigh the decades of exclusivity manufacturers like Amgen achieve as a result of unfair patenting practices in determining the maximum fair price of the selected drugs for Medicare and its enrollees.
Amgen’s Excessive Patenting Practices Will Cost Taxpayers Nearly $2 Billion by 2026
Amgen will presumptively retain rights to exclusively sell Enbrel within the United States, and thereby likely deprive the public of more affordable biosimilars, until 2029.[10] How did the company obtain nearly three decades of exclusivity after the drug’s approval in 1998? Amgen invested in building a fortress of patents around the drug to maintain its monopoly control to the public’s detriment.
Patent protection lasts 20 years from the filing date of the patent application, and in Enbrel’s case, the underlying patent protection in the drug was set to expire in 2019.[11] But, as the Initiative for Medicines, Access and Knowledge (I-MAK) reports, 72% of all patent applications on Enbrel were filed by Amgen after the drug received approval in 1998.[12] By building a wall of patents around one of its top-selling drugs, Amgen successfully thwarted competition from two potential biosimilar competitors, Erelzi and Eticovo, which received FDA approval in 2016 and 2019, respectively.[13] While Americans will be deprived of more affordable biosimilars until 2029, European peers have had access to these more affordable options since 2016.[14]
Public Citizen estimates more than 1 billion dollars in losses to Medicare resulting from the absence of competition from biosimilars to Enbrel.[15] That is, if biosimilars had come to market in 2019 when Amgen’s patent protection in Enbrel was set to expire, Medicare Part D would have spent on a net basis $1,053,023,122 less just on this one treatment by May 2023. As CMS seeks to establish a maximum fair price for Enbrel, it should consider how Medicare and its enrollees lost over a billion dollars in less than four years due to Amgen’s tactics to forestall competition against the drug.
In addition, Public Citizen projects that by the time maximum fair prices for Enbrel go into effect on January 1, 2026, Medicare will have lost nearly 2 billion dollars ($1,891,500,836) due to Amgen’s extended monopoly control of the drug.[16] This estimate is conservative, though, as lost savings were trending upward between 2020 and 2023. CMS should account for the nearly 2 billion dollars Medicare could have saved with competition from biosimilars had Amgen’s patent protection of Enbrel expired in 2019 while it negotiates the maximum fair price for the drug.
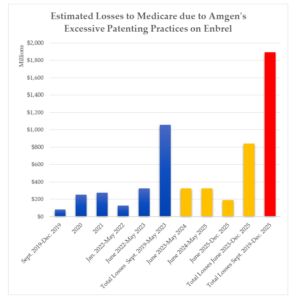
Figure 1. Estimated Current and Projected Medicare Losses Due to the Absence of Competition Against Enbrel (in millions). Current losses to Medicare are indicated in blue. Projected losses to Medicare after June 2023 are indicated in orange. Total estimated losses, combining current losses with projected losses, are shown in red.
Amgen’s Patent Gamesmanship Hinges on Deceitful Contractual Practices
When patent law normally provides only 20 years of protection, it is extraordinary that Amgen will have secured 3 decades of exclusivity from the FDA approval of Enbrel in 1998. Just how did Amgen manage this? Amgen used the cover of contract law to evade limits on its monopoly power over the drug, which will cost the public enormously for years to come. Public Citizen focuses on two of Amgen’s patents and related contracts that have been critical to preventing biosimilar competition.
To provide background for understanding these patents, Enbrel helps treat symptoms of autoimmune diseases by inhibiting the protein, Tumor-Necrosis Factor (TNF), which is key to immune and inflammatory responses. The excessive or inappropriate production of the protein causes the harmful consequences associated with autoimmune diseases, like rheumatoid arthritis.[17] Enbrel, in particular, is a TNF receptor, which binds to and inactivates TNF in order to treat such diseases.[18]
In 1999, Immunex, the original manufacturer of Enbrel, entered into a licensing agreement with Swiss company, Roche, which had also been working on TNF receptors.[19] In 1995, Roche had applied for two patents related to TNF receptors,[20] and the agreement gave Immunex license to those patent applications.[21] But in 2004, after acquiring Immunex, Amgen and these parties entered a new licensing agreement eliminating Immunex’s obligation to pay royalties, paying Roche approximately $45 million, giving Immunex the exclusive right to prosecute the covered Roche patent applications, and providing Immunex the option to convert the license to a complete assignment of rights for a meager $50,000.[22]
Using the authority to prosecute Roche’s patent applications, Immunex amended Roche’s two patent applications to cover etanercept, which Immunex had already claimed in its own patents.[23] Initially, the United States Patent and Trademark Office rejected both of the amended patent applications for being obvious in light of what was known at the time, but the Board of Patent Appeals and Interferences reversed the rejections.[24] More than 16 years after Roche’s initial applications, these patents finally issued in 2011 and 2012.[25] By gaming the patent system through the licensing of Roche’s duplicative patent applications, Amgen was able to win patent protection extending until 2029, a decade after the underlying patent protection was set to expire.
In August 2016, Sandoz received FDA approval for its biosimilar version of Enbrel called Erelzi,[26] but Amgen had commenced a patent infringement action in February 2016 to block the drug from the market.[27] Sandoz defended the lawsuit by trying to invalidate the reworked Roche patents.
In patent law, a party is not allowed to extend the period of exclusivity for its invention by filing a later patent that is not different from an earlier patent the party owns.[28] Sandoz claimed that the reworked Roche patents were indistinct from Immunex’s earlier patents underlying Enbrel.[29] Therefore, the patents were unlawfully extending the exclusivity of the brand name drug. But the district court, and ultimately the United States Court of Appeal for the Federal Circuit in a 2-1 vote, disagreed.[30]
To prove this claim, the challenged patent and the earlier patent must be owned by the same party. However, the Federal Circuit reasoned that the licensing agreement between Immunex and Roche did not transfer all of the substantial rights in the patent applications to Immunex to make it the effective owner of Roche’s patents.[31] The technicality that Immunex owned the earlier patents and Roche owned the later patents meant that Sandoz could not invalidate the patents.[32] In consequence, two patent applications first filed by Roche in 1995 have enabled Amgen to preserve its monopoly until 2029.
The Federal Circuit’s ruling prioritized form over substance: Immunex and Amgen are the effective owners of Roche’s patents and the reworked patents unfairly extend the drug’s exclusivity, as Judge Reyna pointed out in dissent.[33] Any rights Roche retains are illusory since Immunex, at any time, can compel a complete assignment of Roche’s patents for just $50,000.[34] Roche itself was willing to assign all rights to the patents for free, but Immunex was the party that insisted on the provision,[35] presumably to engage precisely in this sort of gamesmanship to undermine legal challenges to its monopoly. The $50,000 is a paltry sum to exercise the option of complete assignment, given that the entire agreement provided Roche $45 million, and Enbrel’s sales were in the billions.[36] Finally, as Judge Reyna noted, the reworked Roche patents are indistinct from Immunex’s earlier patents.[37]
The Federal Circuit’s illogical decision can be summed up by the fact that Amgen and Immunex are the effective owners of Roche’s patents when they earn billions of dollars off Enbrel each year, but they are not effective owners of the patents for the purposes of law. Unfortunately, Amgen’s patent gamesmanship found success again in a second district court ruling centering the same patents, which prevented a different biosimilar, Eticovo, from coming to market.[38]
Amgen’s continued monopoly power over Enbrel reflects a profound failure of the patent system. As CMS seeks to set a maximum fair price for Enbrel in negotiations, the negotiation group should consider the abusive contractual and patent practices the company has engaged in to preserve nearly three decades of exclusivity on the drug.
Recommendations
The Inflation Reduction Act represents a significant step in curbing extensive abuses of pharmaceutical companies in drug pricing. Although Amgen contends that the Act will reduce incentives for innovation, it contributed nothing to the research and development of its blockbuster drug, Enbrel, before its approval in 1998. Further, Amgen gamed the patent system to block price-lowering biosimilar competition from coming to market until at least 2029, which threatens to burden Medicare and its enrollees with nearly 2 billion dollars in unjust costs. The Act now offers CMS an opportunity to fairly recalibrate prices of selected drugs for Medicare enrollees who have been long exploited, and the agency should take full consideration of industry abuses, particularly patent gamesmanship, in reaching a maximum fair price for the drugs.
Public Citizen makes the following recommendations as the negotiation group proceeds with determining a maximum fair price for Enbrel and other drugs under the IRA to constrain the exploitative practices of industry:
- As CMS considers data on pending and approved patent applications and revenue for selected drugs in reaching maximum fair prices, it should weigh patent gamesmanship by manufacturers that unfairly extends exclusivity for these drugs and improperly allows companies to collect exorbitant revenues without adequate competition. Should CMS find, as in the case of Enbrel, that a manufacturer has exploited deficiencies in our patent system to block alternatives from the market, CMS can consider (1) the prices that might be available in the absence of such inappropriate monopoly extensions, and (2) the continued inflated revenues a manufacturer will obtain from its patent abuses. To the extent negotiated prices exceed those that would be available in the absence of unfair monopoly extensions, companies will not be deterred from future misconduct.
- As CMS evaluates research and development costs submitted by manufacturers in negotiating a maximum fair price, companies should not be permitted to pass off inflated acquisition expenditures as research and development costs. Amgen’s $16 billion price tag for acquiring Immunex and the right to manufacture Enbrel did not reflect an intent to reimburse Immunex’s research and development costs in the drug; rather, it reflected the cost Amgen was willing to expend to secure the monopoly power to price the drug as the company wished with minimal constraints. If CMS were to consider these acquisition deals as research and development costs, it will create a perverse incentive for companies to inflate acquisition deals in the future to obtain higher maximum fair prices if Medicare selects their drug for negotiation. Because that artificial price point bears no relationship to research and development costs, CMS should not consider the facial value of acquisition costs in research and development expenditures. Revised guidance for initial price applicability year 2026 indicates that acquisition costs will be included in R&D costs. We strongly urge CMS to qualitatively evaluate these costs differently than more legitimate R&D costs, like clinical trial costs actually incurred. Guidance for future negotiation years should exclude consideration of acquisition costs as R&D expenses.
Additionally, Congress should explore legislation to close loopholes that allow drug corporations to evade appropriate scrutiny over their patents through deceitful licensing arrangements and inappropriately extend monopolies by patenting obvious inventions.
Appendix A: Methodology for Calculating Medicare’s Losses Due to Amgen’s Excessive Patenting Practices
Calculations proceeded in four parts. First, using available data from Medicare and the White House, Public Citizen looked at gross Medicare spending for Enbrel in 2019, 2020, 2021, and from June 2022 through May 2023.[39] Underlying patent protection in the drug was set to expire in August 2019,[40] so Public Citizen calculated savings if biosimilars entered the market for the last third of the year, using a third of the gross spending from 2019. To calculate estimated expenditures from January through May 2022, which is missing from the publicly available data, Public Citizen examined the average monthly spending for Enbrel in the year preceding and the year subsequent to this missing period to determine what spending would likely have been for these five months.
Second, Public Citizen accounted for Medicare’s net expenditures for Enbrel by factoring in potential rebates and discounts from the manufacturer using established figures from academic literature. Specifically, Public Citizen used a 36.8% discount from literature on anti-TNF inhibitors, which aligns with the 37.3% discount found for drugs generally in Medicare Part D.[41]
Third, after estimating Medicare Part D’s net expenditure for Enbrel from September 2019 through May 2023, Public Citizen assumed an 18.4% reduction in price for the treatment based on data on the market entry of biosimilars to Enbrel in Europe.[42] The 18.4% price reduction in Europe was calculated based on ex-manufacturer prices. The ex-manufacturer price is that which is received by the manufacturer of a product and may not account for potential additional rebates or value-based agreements which further decrease the net price available to payers.
Finally, to project how much Medicare will lose before the maximum fair prices for Enbrel go into effect on January 1, 2026, Public Citizen assumed the same losses each year based on the latest period of data (June 2022 to May 2023). Medicare’s loss for that period was $324,572,018.20. To calculate the losses for June 2025 through December 2025, Public Citizen prorated the annual loss for that period. These calculations in lost savings to Medicare do not account for potential increased usage of Enbrel and its biosimilars by Medicare’s enrollees due to lower prices for these treatments from biosimilar competition. Such usage, however, would indicate that Medicare enrollees currently are depriving themselves of necessary treatment due to cost barriers imposed by Amgen.
References
[1] The White House, FACT SHEET: Biden-Harris Administration Announces First Ten Drugs Selected for Medicare Price Negotiation, Statements & Releases (Aug. 29, 2023), https://www.whitehouse.gov/briefing-room/statements-releases/2023/08/29/fact-sheet-biden-harris-administration-announces-first-ten-drugs-selected-for-medicare-price-negotiation/.
[2] Id.
[3] The White House, supra note 1; Assistant Secretary For Planning and Evaluation, Office of Health Policy, Department of Health and Human Services, Inflation Reduction Act Research Series— Medicare Enrollees’ Use and Out-of-Pocket Expenditures for Drugs Selected for Negotiation under the Medicare Drug Price Negotiation Program 2 (2023), https://aspe.hhs.gov/sites/default/files/documents/9a34d00483a47aee03703bfc565ffee9/ASPE-IRA-Drug-Negotiation-Fact-Sheet-9-13-2023.pdf .
[4] See Assistant Secretary for Planning and Evaluation, supra note 3.
[5] See The White House, supra note 3.
[6] Statement on Drug Pricing Provisions Included in “Inflation Reduction Act,” Amgen Newsroom, https://www.amgen.com/newsroom/company-statements/statement-on-drug-pricing-provisions-included-in-inflation-reduction-act (last visited Sept. 21, 2023).
[7] House Oversight & Reform Committee, Drug Pricing Investigation: Industry Spending on Buybacks, Dividends, and Executive Compensation 2 (2021), https://oversightdemocrats.house.gov/sites/democrats.oversight.house.gov/files/COR%20Staff%20Report%20-%20Pharmaceutical%20Industry%20Buybacks%20Dividends%20Compared%20to%20Research.pdf.
[8] Jonathan Gardner, A three-decade monopoly: How Amgen built a patent thicket around its top-selling drug, Biopharma Dive (Nov. 1, 2021), https://www.biopharmadive.com/news/amgen-enbrel-patent-thicket-monopoly-biosimilar/609042/; Justin Gillis, Amgen Agrees to Buy Immunex in Record Biotech Deal, Wash. Post (Dec. 18, 2001), https://www.washingtonpost.com/archive/business/2001/12/18/amgen-agrees-to-buy-immunex-in-record-biotech-deal/fff0293c-a412-4011-8322-49cf15855462/.
[9] Gardner, supra note 8; I-MAK, Overpatented, Overpriced Special Edition: Enbrel (2020), https://www.i-mak.org/wp-content/uploads/2023/01/Overpatented-Overpriced-2023-01-24.pdf.
[10] I-MAK, supra note 9, at 3.
[11] Pet. for Writ of Cert. at 2, Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020).
[12] I-MAK, supra note 9, at 3.
[13] Gardner, supra note 8; Tony Hagen, NJ Court Decision Means 3 Decades of Product Exclusivity for Enbrel, Ctr. for Biosimilars (Dec. 1, 2021), https://www.centerforbiosimilars.com/view/nj-court-decision-means-3-decades-of-product-exclusivity-for-enbrel.
[14] See Elif Car, et al., Biosimilar competition in European markets of TNF-alpha inhibitors: a comparative analysis of pricing, market share and utilization trends, 14 Front Pharmacol. 1 (2023); Samsung Bioepis Enters into Commercialization Agreement for Next-Generation Biosimilar Candidates, News & Releases (Nov. 6, 2019), https://www.samsungbioepis.com/en/newsroom/newsroomView.do?idx=138.
[15] See Figure 1. Appendix A contains the detailed methodology for these calculations.
[16] Id.
[17] Dan-In Jang, et al., The Role of Tumor Necrosis Factor Alpha (TNF-α) in Autoimmune Disease and Current TNF-α Inhibitors in Therapeutics, 22 Int. J. Mol. Sci. 2719 (2021).
[18] More about Enbrel: Mechanism of Action, https://www.enbrelpro.com/more-about-enbrel/mechanism-of-action (last visited Oct. 2, 2023).
[19] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037, at 6 (Fed. Cir. July 1, 2020).
[20] Pet. for Writ of Cert. at 8, Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020).
[21] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037, at 6 (Fed. Cir. July 1, 2020).
[22] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037, 6-8 (Fed. Cir. July 1, 2020); Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020) (Reyna, J. dissenting), at 5.
[23] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020) (Reyna, J. dissenting), at 3-4.
[24] Immunex Corp. et al., v. Sandoz Inc. et al., 395 F. Supp. 3d 366, 379-380 (D.N.J. 2019).
[25] Pet. for Writ of Cert. at 10, Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020).
[26] FDA approves Erelzi, a biosimilar to Enbrel, FDA News Release (Aug. 30, 2016), https://www.fda.gov/news-events/press-announcements/fda-approves-erelzi-biosimilar-enbrel. Because Roche’s two patent applications in 1995 predated the World Trade Agreement on Trade Related Aspects of Intellectual Property Right, which grants patent protection only from the date of filing, the patents received protection under an older rule of 17 years from the date of publication. See Gardner, supra note 8; Immunex Corp. et al., v. Sandoz Inc. et al., 395 F. Supp. 3d 366, 421 (D.N.J. 2019).
[27] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037, at 8 (Fed. Cir. July 1, 2020).
[28] Id. at 9; Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020) (Reyna, J. dissenting), at 2.
[29] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037, at 8 (Fed. Cir. July 1, 2020).
[30] Id. at 3, 15-21.
[31] Id. at 15-21.
[32] Id.
[33] Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020) (Reyna, J. dissenting), at 3-9.
[34] Id. at 4-5.
[35] Id. at 5-6.
[36] Id. at 5.
[37] Id. at 8-9.
[38] Immunex Corp. et al. v. Samsung Bioepis Co., No.: 2:19-cv-11755-CCC-LDW (D.N.J. 2021); Hagen, supra note 13.
[39] See Medicare Part D Spending by Drug- Excel Reports including Historical Data 2021, Data.CMS.gov, https://data.cms.gov/summary-statistics-on-use-and-payments/medicare-medicaid-spending-by-drug/medicare-part-d-spending-by-drug (last visited Sept. 29, 2023); The White House, supra note 1.
[40] Pet. for Writ of Cert. at 2, Immunex Corp. et al., v. Sandoz Inc. et al., No. 2020-1037 (Fed. Cir. July 1, 2020); Immunex Corp. et al., v. Sandoz Inc. et al., 395 F. Supp. 3d 366, 421 (D.N.J. 2019).
[41] See Alvaro San-Juan-Rodriguez, et al., Trends in list prices, net prices, and discounts of self-administered injectable tumor necrosis factor inhibitors, 27 J. Manag. Care Spec. Pharm. 112 (2021); William Feldman et al., Estimating Rebates and Other Discounts Received by Medicare Part D, 2 JAMA Health F. (2021).
[42] See Elif Car, et al., supra note 14.