Waiver of the WTO’s Intellectual Property Rules: Facts vs. Common Myths v 2.0
TRIPS Waiver: Facts vs. Common Myths - Version 2.0
This is part of a Global Trade Watch series on the TRIPS Waiver.
Introduction
More than a year after South Africa and India proposed a temporary waiver of World Trade Organization (WTO) intellectual property (IP) barriers that limit supply of the COVID-19 vaccines, treatments and tests needed to end the pandemic, the WTO was forced to postpone its Ministerial Conference (MC12) after a new, concerning variant, omicron, emerged. WTO member countries’ failure to enact a waiver has contributed to the dangerous situation of only 8% of the population in low-income countries receiving at least one COVID shot, while 65% in rich countries have. In addition to causing avoidable deaths and economic devastation, the shortage of COVID medications in developing countries means raging outbreaks that allow the virus to mutate into new variants, such as omicron.
That the COVID-19 public health disaster and resulting economic crises won’t end anywhere unless people everywhere are vaccinated already was made painfully clear as the delta variant fueled new waves of infection and death around the globe during much of 2021. Governments invested billions to create vaccines. But, there is still a shortage, with no end in sight as children are being vaccinated and adults in developed nations receive boosters.
Today, more than 120 countries, including the United States, support an emergency COVID-19 WTO waiver. But it is actively being blocked by three WTO members: the European Union, led by Germany, plus Switzerland and the UK. As public demand grows for a waiver of the WTO’s Agreement on Trade-Related Aspects of Intellectual Property (TRIPS) rules, Big Pharma is pushing back with old and new myths and lies. Repeatedly, developing countries, public health pundits and civil society experts have debunked these falsehoods. This document brings together these arguments.
The Overwhelming Majority of Developing Countries Have Not Received COVID-19 Vaccines: Don’t Fall for Big Pharma’s Latest Lie About a Glut
Nearly two years into the pandemic and a year after vaccine rollout started in wealthy countries, only 8% of people in low-income nations have received a first shot. Fewer people in eight Southern African countries combined have gotten a first dose than the 38 million U.S. residents that have received a booster. Even so, some have tried to downplay the urgency of increasing supplies of COVID-19 vaccines by noting that South Africa recently asked Johnson & Johnson and Pfizer to suspend delivery of COVID-19 vaccines. To shift focus from the absolute shortfall in vaccine supplies, pharmaceutical interests and their political allies are claiming that vaccine hesitancy and infrastructure problems are the cause of low vaccination rates in developing countries. These claims have been completely debunked.
First, a major issue in South Africa has been the “drip, drip, boom” model by which Pfizer and J&J have delivered vaccines. The firms did not deliver a single shot to South Africa between January and March 2021, slowly started to make shipments in April and then dumped large amounts from July to September. For instance, Pfizer sent almost half of its entire promised 2021 doses for South Africa in those few months. It’s no wonder South Africa would request deliveries be slowed as it works to get most of its entire annual supply into arms in just the last months of the year.
Second, the situation in South Africa, an upper-middle-income country with relative means to pay the gauged prices charged by Big Pharma, is very different from the scenario of low- and lower-middle income countries that have scrambled to find any doses. While most low-income countries have had to rely on subsidized vaccines from COVAX or the scarce donations coming from rich countries to start vaccinating their populations, upper-middle-income countries like South Africa have some resources to negotiate deals directly with pharmaceutical firm to get shots (although often having to accept ignominious conditions related to transparency, liability and pricing). While South Africa would have to spend a non-insignificant 1.5% of its health expenditure to vaccinate 40% of its population, this number rises for low-income countries to 28.5%, according to data from the United Nations Development Programme Global Dashboard for Vaccine Equity. Poorer countries would have to spend more than half of health budgets to vaccinate 70% of their populations if they were to pay the prices that IP monopolies now facilitate.
Third, contrary to Big Pharma claims, the data actually show that vaccine hesitancy is much lower in low- and middle-income countries compared to wealthy nations, such as the United States. A survey conducted between August and December 2020 by the Africa Centres for Disease Control and Prevention and the London School of Hygiene & Tropical Medicine covering 15 African countries (including South Africa) showed that, on average, 79% of Africans would take a COVID-19 vaccine. In contrast, back in January 2021, just 55%, of people on average in high-income countries, such as Canada, Denmark, Germany and France, reported that they either had received a vaccine or were willing to take one, according to Our World in Data figures.
The need for more localized manufacturing is underscored by the monopoly vaccine makers’ practice of not providing doses for months and then dumping of large volumes on developing countries, some with imminent expiration dates, and often without advanced notice. This means countries cannot plan mass vaccination sites and other programs they have been unable to implement for lack of supply. This is not an inherent problem with poor countries’ infrastructure, as has been claimed: The United States also would be hard pressed to administer doses under such conditions. Indeed, public health experts have warned for months that after vaccine makers have kept developing countries at the back of the line for most of the year, suddenly sending millions of doses overnight would stress an already starved system.
Prioritizing vaccine distribution to the Global South would yield high returns in advancing global immunization coverage. As global health advocates have repeatedly asserted, vaccinating developing countries would not only prevent needless death and suffering in these places, but it would benefit the global efforts to end the pandemic.
COVID-19 Vaccine Producers Are Not on Track to Make Enough for Everyone, Contrary to Pharma Company Promises
Pharmaceutical interests have repeatedly claimed that more COVID-19 vaccine manufacturing capacity is not needed because the companies currently holding monopolies on production would manufacture more than 12 billion doses in 2021. (According to some estimates, this was the volume needed to immunize 70% of the world population.)
But, with less than a month remaining in 2021, less than 9.4 billion doses have been produced in the entire world, according to Airfinity data. This means that vaccine makers would have to produce 2.6 billion doses in just one month, which would be almost three times the volume produced in November (around 900 million doses). Hence, once again, the vaccine monopolists likely will not meet their production volume promises. It would not be the first time that industry projections were grossly inflated. In 2020, vaccine manufacturers projected they would make 800 million doses by the end of the year, but in reality produced 20-30 million. In 2021, several vaccine manufacturers faced production issues throughout the year with Moderna recently slashing its annual production volume forecast from an initial 1 billion doses to 700 million. Among the issues have been shortages of vaccine inputs, which are often also caused by IP obstacles, such as production of lipids and other components.
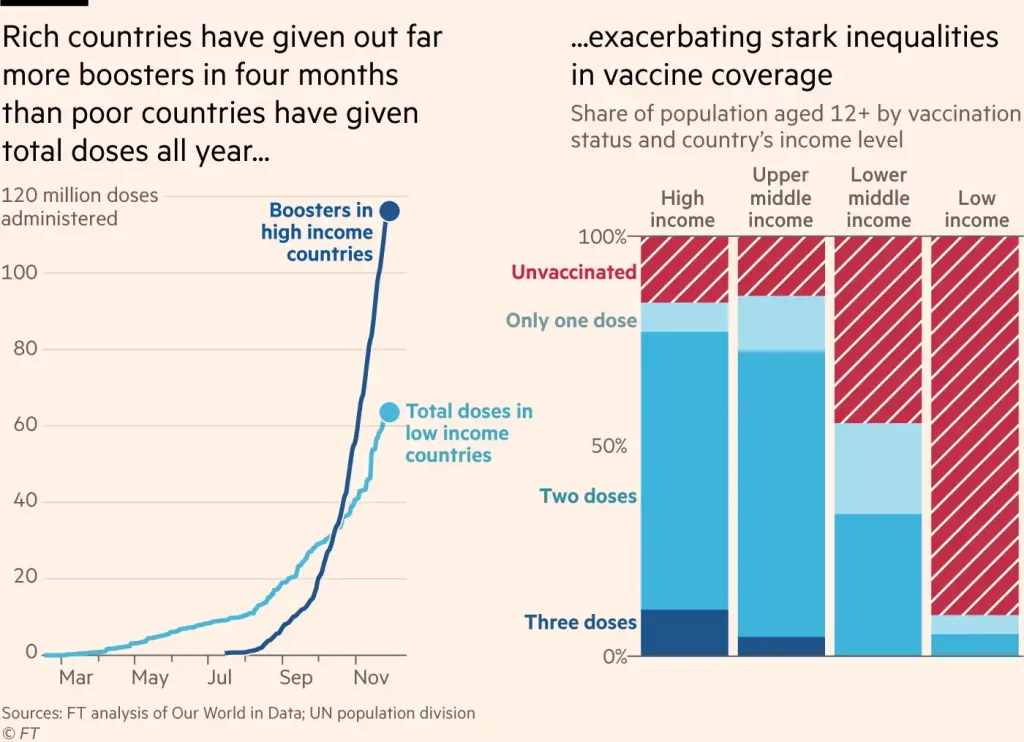
And to make matters even worse, major vaccine producers started prioritizing booster sales at much higher profits in rich countries while billions of people in developing countries have not had initial immunizations. The World Health Organization warned that six times more COVID-19 booster shots are being administered around the world daily than primary doses in low-income countries.
This means that the overall demand is much more likely to lean toward 15 billion doses than the optimistic 11-12 billion mark. And, unless IP barriers are removed so that widespread, decentralized production is incentivized, there might never be massive immunization in poorer countries. Having regions of the world go for years without vaccinations is not only unjust and guarantees preventable deaths and economic pain, but – as the emergence of omicron cautions – increases the chances of vaccine-resistant variants that bear the risk of putting whole world back to square one on immunization. In which case, we will need much more than 15 billion doses if the virus is ever to be tamed. And, these figures do not take into account the possibility that omicron or a future variant will be vaccine-resistant and a new vaccine will have to be administered to everyone who was vaccinated previously. The foreseeable gap in monopoly-holders’ production means that, despite a concerted effort to delay the waiver, it is not too late for this essential intervention.
BioNTech Sold a License to Make the “Pfizer” Vaccine to a Chinese Firm in August 2020 Plus China Has Homegrown mRNA Vacs: So, TRIPS Waiver Can’t Give China “U.S. mRNA Tech”
One of Big Pharma’s absurd claims is that a COVID-19 IP waiver would help China access “U.S. mRNA technology” to create medical innovations. Putting aside the immorality of opposing development of more vaccines and therapeutics on the mRNA platform for cancer and heart disease, the claim is ludicrous. Messenger RNA (mRNA) research has been funded by governments worldwide and has been underway collaboratively in numerous countries for decades. It is not a “U.S. technology.” A Hungarian scientist launched the work in the 1970s. Turkish scientists working in Germany created the BioNTech vaccine that is licensed to Pfizer for production.
Plus, a WTO IP waiver will not transfer mRNA technology to China: A Chinese firm already has the BioNTech-Pfizer COVID-19 mRNA technology. BioNTech, the firm that created the vaccine that is licensed to Pfizer for manufacture and sale in the United States and most of the world, also made a deal for manufacturing and sales in China with Fosun Pharmaceutical in Shanghai. Plus, already there are two indigenous Chinese mRNA vaccines in final trials, including one that can be stored at refrigerator temperature (not ultra-cold like BioNTech-Pfizer-Fosun or Moderna).
A WTO TRIPS Waiver Will Unlock Existing and Potential Capacity in Developing Nations to Gear Up Greater Production of COVID-19 Vaccines, Treatments and Diagnostic Tests
A groundbreaking December 2021 research paper identified at least 120 manufacturers with the technical requirements and quality standards needed to produce mRNA vaccines across Asia, Africa and Latin America. The health experts conducting the research concluded that with the appropriate tech transfer these companies could manufacture mRNA shots, just as firms in the global North with similar profiles have done after mRNA vaccine developers contracted with them to scale up the developers’ production. While the number of prospective producers is notable, that there are many qualified firms in the Global South that could be expanding mRNA vaccine supplies. Two months earlier, a New York Times exposé spotlighted 10 companies headquartered in developing countries that are strong candidates to manufacture mRNA vaccines considering their existing facilities, human capital, and the regulatory system for medicines and political and economic climates of the countries in which they are based. And, back in March 2021, a group of medicine-production experts in a Foreign Policy article noted that, just in Africa, “Biovac and Aspen in South Africa, Institut Pasteur in Senegal, and Vacsera in Egypt could rapidly retool factories to make mRNA vaccines.”

Source: Human Rights Watch
Additionally, the Serum Institute in India already is manufacturing the AstraZeneca shot and is poised to make Novavax vaccines, while Moderna declined to partner with a qualified Bangladeshi vaccine maker, claiming its engineers were too busy to focus beyond U.S. and EU production. Likewise, Moderna rejected the World Health Organization (WHO) calls to contribute to the creation of regional mRNA vaccine manufacturing hubs both in Africa and South America.
The few firms now maintaining monopoly control over the effective vaccines tout agreements they have made for firms in developing countries to “produce” COVID-19 vaccines. However, most of these arrangements are “fill and finish” late-stage manufacturing, which do not entail production of the actual vaccine substance. Thus, these arrangements do not require significant tech or know-how transfer. Not a single mRNA vaccine developer has granted a manufacturing license to a company in the Global South that grants access to the vaccine recipe.
Yet, the existing and planned contract manufacturing arrangements prove facilities in developing countries certainly can produce COVID-19 vaccines. But unless technology and know-how are shared more openly, the monopoly holders w ill maintain absolute control over how much can be produced, what the price is and where it will be sold. This was painfully demonstrated when South Africa’s Aspen Pharmacare was required to export to Europe most of the Johnson & Johnson COVID-19 vaccine it produced when locals needed the shots the most. Similarly, the Serum Institute is barred from supplying upper-middle-income and high-income countries with the AstraZeneca vaccines it makes, meaning AstraZeneca artificially segmented the global market to ensure that it is the only supplier of the Oxford vaccine in the most profitable national markets, according to Doctors Without Borders.
Scores of countries are ready to invest in building new or repurposing existing facilities to create independent production capacity. That is why more than 120 countries support a TRIPS waiver. These countries seek certainty that if they adjust their domestic laws and practices to support that investment by providing access to the necessary technology, they will not get dragged into expensive WTO litigation or face retaliatory sanctions from countries claiming WTO violations. The waiver will also serve as a worldwide buffer against the political pressure and legal harassment to which Big Pharma subjects countries that seek to promote affordable access to medicines.
In many countries, the regulatory authorities that had to approve domestic use of various vaccines and other COVID-related medical products have significant information from the firms that they could share with skilled teams from local universities, government agencies and pharmaceutical manufacturers — if they were not obliged by WTO rules to guarantee monopoly control of it. And world class pharmaceutical firms already are making generic versions of new cutting-edge HIV/AIDS medicines and pumping out vaccines based on the platform that, for instance, the Johnson & Johnson vaccine uses.
At issue is not manufacturing capacity or skills, but rather control: Big Pharma has a monopoly over vaccine knowledge and technology platforms that will determine life and death for millions of people in rich and poor countries alike and decide the fate of the global economy. These corporations stand to make a lot of money. Pfizer and Moderna recently revealed COVID-19 vaccine expected revenue of $36 billion and $18 billion respectively in 2021 alone. Speaking at the virtual Barclays Global Healthcare Conference in mid-march 2021, Pfizer’s senior VP of investor relations described how the firm planned to raise prices and profit richly by selling vaccines annually to rich countries that can pay. Big Pharma firms may have no interest in sharing the vaccines created thanks to billions in taxpayer funding. But the health and economic futures of billions of people around the world require urgent access to the formulas and technology needed to massively scale up production worldwide for use in every corner of the globe.
Speedy Creation of COVID-19 Vaccines and the Innovations Underlying Them Were Made Possible by Billions in Taxpayer Funds, Not by IP Protections
The standard Pharma claim is that their monopoly rights and high prices are necessary to support innovation. But the speedy development of COVID-19 vaccines proves the opposite point: Every leading COVID vaccine, on the market or in final clinical trials, has benefited from substantial public investment. The miracle of speedy COVID vaccines resulted from taxpayers providing pharmaceutical firms billions to develop and test COVID-19 vaccines and then billions more in pre-orders, not from pharmaceutical firms investing monopoly-gained profits. By one estimate, during the pandemic governments already have transferred more than $112 billion to pharmaceutical firms, mainly for COVID-19 vaccine development. Before that, the U.S. National Institutes of Health (NIH), military and other agencies invested in coronavirus research for decades. Governments have invested our tax dollars far more than pharmaceutical corporations have spent their own funds in developing these medicines. Why should pharma corporations have monopoly control over COVID-19 vaccines they took little risk or expense in developing?
Indeed, the COVID vaccine situation proves the opposite point that Big Pharma interests claim. This is the third time in the last 20 years that a coronavirus has made the leap from animals to humans: Sars coronavirus in 2002, Mers coronavirus in 2012, and Sars-CoV-2 in 2019. Yet the patent protections of the pharmaceutical industry have yielded little investment in our pandemic preparedness. Why? “Because there is no real incentive to do this, no financial incentive,” Johnson & Johnson’s chief scientific officer admitted. Under our current IP paradigm, firms that did not use past profits from their monopolies to prepare for the next outbreak obtained billions in public dollars to develop vaccines for this crisis. They are given absolute control over the production and distribution of these drugs that will literally determine who lives and dies and the fate of the global economy.
Adopting a Meaningful TRIPS Waiver is an Urgent, Critical Step to Ending the Pandemic
As the emergence of the omicron variant shows, as long as there are raging outbreaks anywhere, COVID-19 will mutate and the possibility of more infectious or deadly strains increases. That’s why, unless people everywhere are vaccinated, we face the prospect of an endless pandemic. And, a critical step to launch a true global vaccination plan is removing the WTO IP barriers limiting vaccine production around the world. Additionally, rich country governments that host vaccine originators must leverage their legal authority to compel technology and know-how transfer, and mobilize sufficient resources to create widespread, decentralized global vaccine production.
Indeed, a former Moderna director of chemistry revealed that with enough technology transfer and know- how-sharing, a modern factory should be able to get mRNA vaccine production online in, at most, three to four months. Others have different estimates, but the important point is that if a TRIPS waiver is not enacted before the end of 2021, the world risks spending most of 2022 worrying about the emergence of the new variant that would take us back to square one in the fight against COVID-19 and, what is even worse, without learning any lessons of the 2021 vaccine apartheid.