Mpox Vaccine Shortfall
Jynneos (MVA-BN) Still Priced at a Premium
By Megan Whiteman
The MVA-BN mpox vaccine (marketed as “Jynneos” by Bavarian Nordic) is in short supply for the ongoing emergency response in Africa. On June 5, 2025, Africa CDC’s Dr. Ngashi Ngongo identified MVA-BN’s high price as “one of the major bottlenecks” to meeting supply needs.
In October 2024, health groups called on Bavarian Nordic to quarter the vaccine’s price and increase the doses available to UNICEF in order to avoid artificial supply scarcity. The company has not replied to the letter or publicly justified its pricing.
UNICEF lacks funding to secure roughly 350,000 doses remaining from its one million dose supply agreement.[1] Moreover, the Africa CDC estimates that the region requires 6.4 million doses to help contain the outbreak and target endemic areas. Apart from UNICEF’s doses, the Africa CDC reports that 219,540 MVA-BN doses pledged by the U.S. could be made available, provided the U.S. government authorizes their release. The Trump administration illegally dismantled the United States Agency for International Development (USAID)—the agency had been helping facilitate the transfer of vaccines—and stopped working with the World Health Organization (WHO), that, along with other partners, is organizing vaccine allocation for the response. These actions have made the delivery of these doses—and potentially as many as 695,000 more U.S.-pledged doses—uncertain[2] and have more broadly prompted a concurrent crisis of disrupted care and severe funding shortfalls across a range of disease areas and health services.
Even if both the UNICEF doses and U.S. doses are made available, between 2.8 million and 5.8 million doses would still be needed to meet the Africa CDC’s estimated need, depending on how Africa CDC accounts for doses of the separate LC16m8 vaccine to be made available to the Democratic Republic of the Congo (DRC).[3] Additionally, in the absence of more affordable options, MVA-BN’s high price will continue to constrain vaccine supplies for potential future mpox outbreaks or for use in areas where mpox is endemic.
Limited vaccine availability complicates supply allocation between and within countries and can severely reduce the scope and ambition of vaccination plans. For example, by the end of May, Sierra Leone had reported nearly 3,000 mpox cases in 2025 but had so far received only 58,000 vaccine doses[4] —enough for an extremely targeted vaccination campaign. At that caseload, a broader, but still targeted, campaign (including both primary and secondary case contacts and at risk groups) could require as many as 600,000 doses.[5]
MVA-BN’s unaffordable, unjustified price
In August 2024, Bavarian Nordic’s vice president of investor relations stated that it was “very unlikely that any African country will ever be responsible for buying vaccines.” Instead, he said, “[v]accines to Africa will come from donations from organizations and countries.” But Bavarian Nordic also has a responsibility to remedy its approach to pricing and access and to help address the shortfall.
Early on in the emergency, Bavarian Nordic made assurances that it could provide as many as 13 million doses by the end of 2025 for the response, provided orders were placed. But at the same time, the company has priced MVA-BN out of reach for many African countries and for organizations that could purchase additional doses on their behalf. UNICEF and Gavi openly acknowledged that MVA-BN’s “high-cost per dose, and the need for a two-dose regimen, could impact the amount of vaccines Gavi and UNICEF can purchase and ultimately the number of people reached and potentially even our ability to stop this outbreak.”
MVA-BN’s inexplicably high price tag:
- Bavarian Nordic sold MVA-BN to UNICEF for $65 per dose—making it the second-most expensive vaccine that UNICEF procures and 26 times more expensive than the median price of UNICEF-procured vaccines. Additionally, the U.S. appears to have paid less than UNICEF to stockpile MVA-BN, raising questions about why a significantly lower price was not offered to poorer nations and those like UNICEF procuring doses for the emergency response.
- Bavarian Nordic’s pricing and lack of transparency are even more egregious considering that public funding underpins the development of MVA-BN[6] and sustains Bavarian Nordic’s long-term sales. As of May 2025, the U.S. government has committed over $2.4 billion to the development and procurement of MVA-BN.[7]
- Bavarian Nordic’s sales have increased exponentially in recent years. Between 2022 (the first year that the WHO declared an mpox emergency) and 2024, Bavarian Nordic has seen a 523% increase in cumulative revenue from MVA-BN compared to the previous three years (2019–2021).[8] Increased sales and long-term stockpiling agreements with high-income countries should give Bavarian Nordic more flexibility to lower MVA-BN’s price.
In addition to offering an affordable price for MVA-BN, Bavarian Nordic should share technology and know-how with developing country manufacturers to expand affordable supply. In December 2024, Bavarian Nordic entered into a technology transfer and licensing agreement with the Serum Institute of India. However, based on limited publicly-available information about the agreement, it appears that Bavarian Nordic will retain control over the supply and price of MVA-BN outside of India.
Enduring Inequity
During a different mpox outbreak that began in 2022, rich countries held the overwhelming majority of scarce MVA-BN supplies, despite significant caseloads in other countries. African countries, including those where mpox is endemic, obtained zero doses at the time. Now, African countries represent the majority of global mpox cases,[9] yet still lack sufficient access to vaccines. Unlike the 2022/3 emergency, global MVA-BN supplies are not scarce. Bavarian Nordic has the capacity to increase supplies. But additional doses are priced out of reach, keeping vaccine availability artificially constrained.
We compared the current mpox vaccine supply situation in Africa to supply in just the U.S. during the previous mpox emergency. At around the same point in the 2022/3 emergency (~9 months in), the U.S. alone had 5.7 times more doses available (with millions more still to be delivered) compared to the current unallocated supply available for the response in Africa.[10] For every one case in the U.S. at that time, there are currently 69 confirmed cases in Africa (this likely understates the disparity considering testing gaps in some countries).[11]
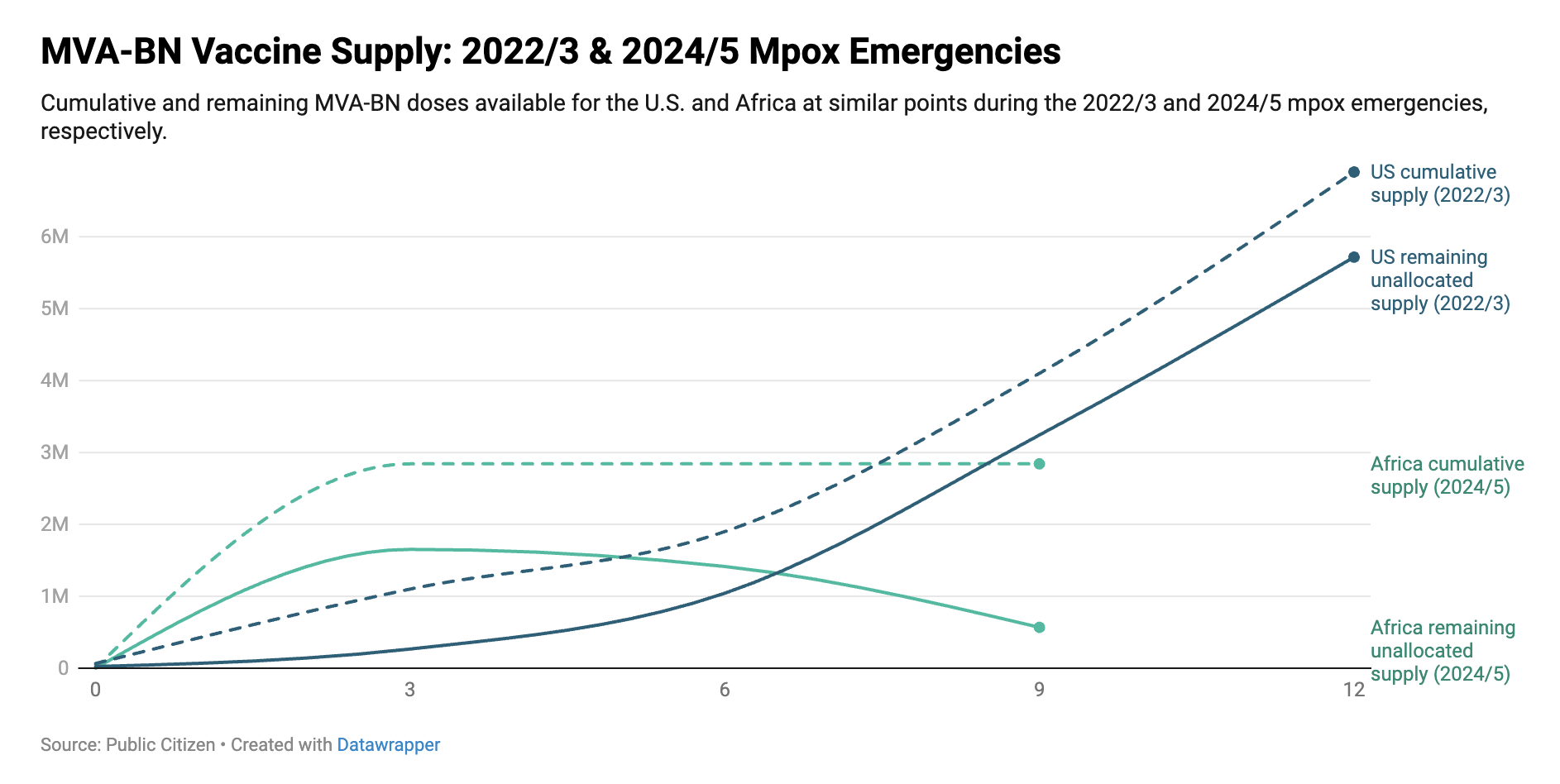
Figure: MVA-BN vaccine supply (in vials) at similar points (defined by the number of months the emergency response has progressed) in the 2022/3 and 2024/5 mpox emergencies.[12]
By spring 2023, cases were falling in the U.S. and vaccine uptake slowed. Nonetheless, the available supply of vaccines in the U.S. would continue to increase as ordered doses were delivered throughout the year. Contrast this with the current outbreak in Africa, where several countries have been allocated doses and ramped up deployment in recent months but supplies remain limited and long-term supply uncertainties persist. This artificial scarcity suppresses the ambition of vaccination programs and recommendations, at national and regional levels. Had Bavarian Nordic set a reasonable price for MVA-BN from the start of the emergency, the supply situation in Africa might look different.
In its global mpox response plan, the WHO recommends that mpox vaccine manufacturers consider reviewing their access and pricing policies to ensure vaccines are accessible and affordable in low- and middle-income countries in a timely manner for immediate and future vaccine needs. To that end, Bavarian Nordic should substantially lower MVA-BN’s price, increase the supply available to UNICEF, and share the information and materials necessary to diversify mpox vaccine producers. Doing so will help protect affected communities, contain outbreaks, and lower the risk that mpox spread poses to everyone.
References
[1] Africa CDC, Special Briefing on Mpox and other Health Emergencies (May 29, 2025), https://www.youtube.com/watch?v=98e23oG3x-4, at 25:40
[2] According to the Africa CDC, 219,540 doses from the U.S.’s pledge are “available”, provided authorization is obtained. However, it appears that an additional portion of the pledge has gone unfulfilled. To our knowledge, the mpox Access and Allocation Mechanism has only allocated 305,000 doses from the U.S. pledge for distribution to African countries. If the unreleased doses that the Africa CDC referred to are from this first tranche (which may have been allocated but not yet delivered), then nearly 700,000 doses remain from the pledge—in addition to the 219,540 doses that the Africa CDC mentioned. One recent report states that about 500,000 doses from the U.S. pledge have arrived for the response, though we could not confirm this based on other public reports.
[3] Depending on how the Africa CDC has accounted for the three million doses of the LC16m8 vaccine being made available via a bilateral donation between the government of Japan and the Democratic Republic of the Congo. To our knowledge, DRC is the only country in the region to have authorized the LC16 vaccine.
[4] Africa CDC, Special Briefing on Mpox & other Health Emergencies, (May 22, 2025), https://www.youtube.com/watch?v=y14EKsdJ4qI, at 37:40.
A second, smaller dose allocation was also recently announced for Sierra Leone.
[5] Africa CDC, Mpox Continental Response Plan 2.0 (Apr. 15, 2025), https://africacdc.org/download/mpox-continental-response-plan-2-0/, at 28 (noting vaccination coverage targets include of contacts of cases (estimated at about 20 per case), contacts of contacts (estimated at about 200 per case), and at risk populations). The 600,000 dose estimate assumes a single-dose strategy. The dose requirement would be double if a two-dose strategy were used.
[6] For a detailed narrative on the public contributions to MVA-BN’s development, see Rizvi, How a Danish Company Grabbed Control of the Monkeypox Vaccine, The American Prospect (Sept. 22, 2022), https://prospect.org/health/how-danish-company-grabbed-control-of-monkeypox-vaccine/
[7] For details of U.S. support through October 2024, see Whiteman & Maybarduk, Mpox Vaccine Access, Public Citizen (Oct. 1, 2024), https://www.citizen.org/article/mpox-vaccine-access/. Funding commitments made between October 2024 and May 2025 retrieved from USAspending.gov.
[8] MVA-BN revenues retrieved from Bavarian Nordic’s 2019–2024 annual reports.
[9] WHO, 2022-24 Mpox Outbreak: Global Trends, https://worldhealthorg.shinyapps.io/mpx_global/#trends-in-cases (accessed June 1, 2025).
[10] Currently remaining MVA-BN doses for the response in Africa refers to the “available” doses reported by the Africa CDC (i.e. the approximately 350,000 doses remaining in UNICEF’s supply order and the approximately 220,000 U.S.-pledged doses reported by the Africa CDC as available but in need of U.S. authorization). Remaining doses available in the U.S. during the 2022/3 emergency were calculated based on publicly available information on MVA-BN orders, deliveries, and allocations to U.S. states.
[11] Cases over a one-month period. According to WHO data, there were 49 confirmed cases in the U.S. in March 2023 and 3,371 confirmed cases in the African region in April 2025 (the most recent month with complete data at the time of writing).
[12] Cumulative supply for Africa represents total purchased or pledged MVA-BN doses for the 2024/5 response (this does not capture any potential loss due to uncompleted pledges). The value for cumulative MVA-BN doses for Africa is based on Public Citizen’s count of doses pledged and purchased for the response from the U.S., Canada, the EU, several European countries, Bavarian Nordic, and Gavi/UNICEF. Our total count is similar to those reported in Think Global Health and by the WHO.
“Available” supply for the African region represents unallocated doses (calculated as total doses pledged or purchased for the response minus allocated doses). The currently available supply is presented as reported by the Africa CDC (this includes doses remaining in UNICEF’s order as of May 29, 2025 and approximately 220,000 doses pledged by the U.S. government).
“Available supply” for the U.S. represents doses available in the country minus doses allocated to states (as reported by the U.S. government (ASPR) at the time).
The figure does not include the three million LC16m8 doses pledged by the government of Japan to DRC as part of a bilateral arrangement (though these doses have recently started to arrive in DRC, which the Africa CDC states should help bolster supply in DRC).