The Fate of Flu
U.S. Plan to Withdraw from the World Health Organization Raises Critical Questions About Flu Preparedness & Response
By Megan Whiteman
Each year, the World Health Organization (WHO) convenes experts to analyze data on global flu virus circulation and make recommendations for the composition of the seasonal flu vaccine, as well as recommendations related to pandemic preparedness. U.S. institutions participate in this convening as part of their broader roles within a global flu surveillance and response network that benefits the U.S. and the world. The U.S. must fully engage in global disease surveillance and response to protect the public.
Key Points
- U.S. participation in WHO’s Global Influenza Surveillance and Response System (GISRS), a collaborative model led by the WHO for sharing viruses and data, bolsters U.S. preparedness.
- The U.S., recognizing the benefit of enhancing flu surveillance capacity in countries to help understand viral spread and stop novel flu outbreaks at their source, has provided technical support, training, materials, and funding directly to other countries to strengthen this network. This can help prevent diseases from spreading abroad, including to the U.S.
- Beyond flu, GISRS provides vital infrastructure for broader disease surveillance and response by enhancing capacities to detect and respond to other viruses with pandemic potential or pandemic variants that can make pandemics harder to contain. For example, during the COVID-19 pandemic, the GISRS network was leveraged to enhance response.
- WHO vaccine recommendations guide national decision-making on the composition of seasonal flu vaccines.
- U.S. institutions play an active role in sharing and analyzing flu virus data and in the WHO-led consultation to select the optimal composition for seasonal flu vaccines. The U.S. Food and Drug Administration (FDA) uses the WHO recommendations as a guide for national recommendations on vaccine composition. This helps enable the development of effective seasonal flu vaccines for the U.S.
- Seasonal flu vaccine manufacturing follows a tight timeline. Any delay in selecting the strains for next year’s U.S. flu vaccine could significantly impact U.S. supply and delivery.
- U.S. disengagement from global flu surveillance and response could have far-reaching consequences.
-
GISRS’ overall capacity will be hampered leading to potentially less effective and less timely vaccines, and leaving the world more vulnerable to pandemic threats.
-
- The Trump administration’s short-sighted plan to withdraw from WHO leaves unanswered critical questions about our ability to respond to infectious disease threats.
Introduction
On February 12, 2025, WHO reported that the United States Centers for Disease Control and Prevention (CDC) had stopped sharing seasonal flu data with WHO global surveillance platforms and had ceased direct communications with WHO related to seasonal flu.[1] These actions raised concerns about whether U.S. institutions would participate in this week’s WHO-led convening to analyze flu data and select the optimal composition for flu vaccines. On the first day of the convening, CDC confirmed that it and the U.S. FDA would be participating. Despite this, questions remain about broader participation in important flu surveillance and control activities.
This all follows an executive order announcing the intent to withdraw the U.S. from WHO (a process that takes one year), pausing the transfer of U.S. government funds, support, and resources to WHO, and recalling U.S. government personnel or contractors working with WHO.[2] The administration subsequently sent a memo to public health officials at CDC directing them to stop communicating with WHO.[3]
Since 1952, WHO has coordinated global flu surveillance through GISRS—a network of institutions dedicated to monitoring and controlling flu.[4]
The GISRS network is a global mechanism for flu surveillance, preparedness, and response. For decades, CDC and other U.S. institutions have supported GISRS’ mission to protect people, including Americans, from seasonal and pandemic flu.
There have been several flu pandemics throughout history. The worst recorded began in 1918 and is estimated to have infected 500 million people and to have killed as many as 50 million people worldwide.[5] Most recently, the world responded to a pandemic flu in 2009 that was first detected in California.[6] The U.S. has invested heavily to prepare for potential flu pandemics.[7]
Aside from the threat of pandemic flu, each year, there are around one billion cases of seasonal flu.[8] Seasonal flu can cause mild to severe illness, and can sometimes lead to death.[9] In the U.S., according to CDC estimates, last year alone flu was associated with 40 million illnesses, 18 million medical visits, 470,000 hospitalizations, and 28,000 deaths.[10]
Vaccines are the primary method to prevent and lower the risk of harm from seasonal flu.[11]
WHO is the global linchpin coordinating the highly technical and collaborative process to help ensure flu vaccines are as effective as possible. This WHO-coordinated effort demonstrates how the U.S. and other WHO member states benefit from and contribute to WHO mechanisms to maximize returns—achieving far more together than any one country could on their own.
In this report, we provide a brief overview of GISRS and some of the U.S. support for strengthening GISRS. Then, we outline the steps involved in ensuring the timely delivery of appropriate seasonal flu vaccines each year. Finally, we discuss how U.S. disengagement from WHO/GISRS could impact seasonal and pandemic flu surveillance and control.
The WHO Global Influenza Surveillance and Response System
GISRS is a global network of public health institutions coordinated by WHO that operates year-round surveillance, sharing information and virus materials to protect people from the threat of flu.[12] These institutions include 152 National Influenza Centres (NICs), 7 WHO Collaborating Centres for Influenza (CCs), 4 WHO Essential Regulatory Laboratories (ERLs), and 12 WHO H5 Reference Laboratories across 130 WHO member states.[13] GISRS serves as a global mechanism of surveillance, preparedness, and response for seasonal flu and flu viruses that could cause pandemics.[14]
In brief, GISRS:
- Helps countries to promptly detect and share flu viruses within the global network. The subsequent characterization of these viruses is essential to assess which viruses are expected to circulate in upcoming flu seasons or have the potential to cause a future pandemic.[15]
- Provides information-sharing and analysis platforms. The GISRS network provides updates on global flu circulation through the analysis of laboratory and disease surveillance results reported through the WHO FluNet and FluID platforms.
- Recommends viruses—based on the information shared among GISRS members—for inclusion in seasonal flu vaccines and in vaccines for pandemic preparedness or response.
- Produces and distributes materials necessary for the production and approval of flu vaccines.[16]
- Provides guidance, support, and materials to labs to strengthen surveillance capacities.[17] These activities include updating and providing diagnostic tests and supporting surveillance of antiviral drug resistance.[18]
U.S. institutions hold several roles within GISRS. The U.S. CDC’s Influenza Division serves as both a flu collaborating center and H5 reference laboratory. There is a second U.S.-based flu collaborating center (St. Jude Children’s Research Hospital) that specifically focuses on the threat to humans from animal flu viruses.[19] The U.S. FDA Center for Biologics Evaluation and Research is an essential regulatory laboratory within GISRS.
The network’s capacity has grown substantially over time. Between 2014 and 2019, GISRS tested an average of 3.4 million flu specimens annually.[20] This has increased to 6.7 million tests annually in recent years.[21] The network shares around 20,000 viral samples with WHO flu collaborating centers (including the U.S. CDC) each year.
The monitoring and analysis of changing flu viruses informs timely risk assessment of flu threats and helps ensure that seasonal flu vaccines are well-matched to circulating strains. GISRS’ large global network, which facilitates data sharing and collaboration across countries, is essential to this “matching” effort. A significant mismatch between the strains targeted in vaccines and those circulating during flu season may mean vaccines will not offer optimal protection against flu.[22]
Box 1 shows slides presented at the two most recent FDA advisory committee meetings for selecting the flu strains to be included in U.S.-licensed vaccines. A representative from CDC’s WHO collaborating center presented the top two images showing flu viruses shared through GISRS’ large network. The third image is a slide from the Department of Defense (DoD) on international flu data to inform the U.S. selection process—showing a smaller footprint than that of GISRS. The slide explains that DoD’s Global Emerging Infections Surveillance network complements, rather than replaces, WHO efforts.
Box 1. FDA Vaccines and Related Biological Products Advisory Committee (VRBPAC) Meeting, March 5, 2024 and October 10, 2024: CDC CC and DoD Slides.
 March and October 2024 VRBPAC presentation slides from CDC’s WHO flu collaborating center show the GISRS network sharing flu viruses with flu collaborating centers during the specified time periods. March 2024 VRBPAC presentation slide from DoD shows the GEIS network’s international surveillance (DoD did not present at the October 2024 VRBPAC meeting). Top left: CDC CC, March 2024; Top right: CDC CC, October 2024; Bottom: DoD, March 2024.
March and October 2024 VRBPAC presentation slides from CDC’s WHO flu collaborating center show the GISRS network sharing flu viruses with flu collaborating centers during the specified time periods. March 2024 VRBPAC presentation slide from DoD shows the GEIS network’s international surveillance (DoD did not present at the October 2024 VRBPAC meeting). Top left: CDC CC, March 2024; Top right: CDC CC, October 2024; Bottom: DoD, March 2024.
U.S. Support Helped Fortify the Foundations of Global Flu Prevention and Control
The U.S. has leveraged WHO mechanisms to expand participation in GISRS. For example, in 2004, CDC entered into cooperative agreements with nine countries, providing funding, training, and technical assistance to strengthen their respective surveillance capacities.[23] Countries were eligible to enter into these agreements on the condition that they had a WHO-designated national influenza center (NIC) and thus had agreed to WHO’s terms of reference, committing to share flu data and viral samples through GISRS.[24] In 2006, CDC expanded its bilateral program to 29 countries and extended the scope of its agreements to include helping counties without NICs to establish them.[25] By 2022, the CDC’s international program had provided technical and financial assistance to bolster flu prevention and control in over 70 countries.[26]
CDC also produces and provides diagnostic reagents to labs to support year-round surveillance capabilities. Diagnostic reagents and protocols for global virus detection are regularly updated based on viruses shared within the GISRS network. This helps the network identify the types of flu viruses that are circulating and alert for those that may have pandemic potential.[27] Similarly, CDC (and other flu collaborating centers and essential regulatory laboratories) produce materials necessary for flu vaccine production, including candidate vaccine viruses and potency reagents.
In 2008, CDC established the International Reagent Resource (IRR) as a warehouse for CDC-developed flu materials that laboratories around the world use to develop diagnostics, vaccines, and drugs and to conduct flu surveillance.[28] The IRR is operated by the American Type Culture Collection under contract with CDC.[29] Participation requires registration and materials are provided after CDC approval is granted.[30] According to CDC, in 2017, 83% of international labs participating in WHO’s GISRS were registered with IRR.[31]
U.S. Seasonal Flu Vaccine Selection and Production
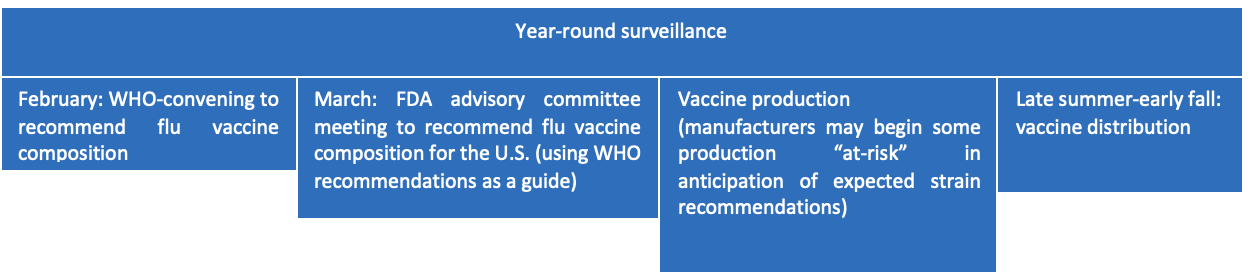
The figure below outlines the general process leading to the distribution of seasonal flu vaccines in the U.S. each fall.[32]
Surveillance and virus sharing
The GISRS network enables the collection of information on a large scale which allows WHO and partners to detect and analyze seasonal flu strains that are circulating.[33]
National labs within GISRS collect virus specimens and perform preliminary analysis in countries all over the world. The labs report data as often as every week through WHO online platforms including FluNet and FluID.
There are several other responsibilities set out in the WHO terms of reference for GISRS labs that require sharing of representative seasonal flu virus isolates and/or clinical specimens, as well as any unsubtypable flu viruses, with the WHO flu collaborating centers.[34] With support from the US, among others, WHO provides financial and logistical assistance to low- and lower-middle income countries to support prompt sharing of flu viruses with the global network.[35]
Once received, WHO flu collaborating centers (including the U.S. CDC) perform a more detailed characterization of these viruses. This analysis informs the selection of vaccines for seasonal flu.
Selecting viruses to target in seasonal flu vaccines
Around February each year, WHO convenes experts (consisting of GISRS members and other relevant parties) to analyze flu surveillance data generated by the GISRS network and issue recommendations on the composition of vaccines for the upcoming Northern Hemisphere flu season (the group repeats this process in September to recommend vaccine composition for the Southern Hemisphere).[36]
Shortly after the WHO meeting, FDA convenes the Vaccines and Related Biological Products Advisory Committee (VRBPAC) to recommend the flu viruses that should be included in FDA‐licensed vaccines for the next flu season, using the WHO recommendations as a guide.[37] This meeting includes additional input from CDC, DoD, manufacturers, and the public.
Making and distributing vaccines
The manufacturing process for the majority of flu vaccines takes approximately six months from the time WHO and VRBPAC recommendations are made.[38] However, manufacturers may begin manufacturing some vaccine components “at risk” in anticipation of likely recommendations, in order to ensure enough vaccine can be delivered in time for the upcoming flu season.[39] If the strain produced at risk differs from the ultimate recommendations, this material is unusable and new product must be produced.[40]
GISRS institutions (collaborating centers and essential regulatory laboratories—including those within the U.S. CDC and FDA) make available candidate vaccine viruses and reagents needed for seasonal flu vaccine production to manufacturers.[41] CVVs are viruses prepared for potential use in vaccine manufacturing.[42] As a regulatory lab within GISRS, the U.S. FDA prepares potency reagents to ensure uniform standards and product consistency.[43]Both vaccine manufacturers and FDA use these standardized reagents for testing, quality control, and release of seasonal flu vaccines.[44]
Manufacturers then submit their vaccine testing results and provide samples from each lot to the U.S. FDA before vaccines can be released.[45]
In summary, the selection and manufacturing of seasonal flu vaccines currently relies on interdependent processes involving WHO/GISRS, manufacturers, and the FDA.
Critical Questions About U.S. Disengagement from Global Flu Surveillance and Response
The Trump administration has introduced significant uncertainty into standard U.S. public health processes, leaving several questions about seasonal flu response unanswered. Sustained U.S. disengagement from global flu surveillance and response raises further questions about America’s ability to respond to seasonal and pandemic flu.
1. Does the U.S. have a plan for the selection and production of seasonal flu vaccines this year?
After ceasing communications with WHO in accordance with Trump administration orders, the U.S. CDC and FDA confirmed that they would participate in the WHO-led process to analyze global flu data and select seasonal flu strains for vaccines to target. Given that the U.S. uses WHO recommendations to guide domestic decision-making on the composition of seasonal flu vaccines, it is important that the U.S. CDC and FDA are participating in this process.
Questions remain around whether deviation from other important processes related to the selection and production of seasonal flu vaccines are to be expected.
- Will FDA’s VRBPAC be permitted to meet in March? Since the start of the Trump administration, many advisory committee meetings have been canceled.[46] As of February 25, 2025, no VRBPAC meeting date to recommend U.S. flu vaccine composition had been announced[47] (typically, dates are announced several weeks in advance). Beyond potential changes to vaccine composition, a delay in the recommendation timeline could disrupt already tight vaccine production schedules.[48] According to the CDC, U.S. seasonal flu vaccine demand peaks in October or November and a mismatch in production timelines can impact vaccine availability and uptake.[49] Another committee—CDC’s Advisory Committee on Immunization Practices (ACIP)—meets in late summer to develop guidance on the appropriate use of seasonal flu vaccines, including on timing of administration and recommended populations.[50] Notably, the ACIP meeting planned for February has been postponed and no new date announced.[51] Disruption to either VRBPAC or ACIP meetings could ultimately impact seasonal flu vaccine access.
- Have the U.S. CDC and FDA fully resumed their other activities as part of the GISRS network? For example, beyond participating in the WHO consultation, CDC and FDA, as part of GISRS, also develop and provide candidate vaccine viruses[52] and potency reagents that are necessary to produce seasonal flu vaccines.[53] However, not all materials are necessarily available from all WHO flu collaborating centers or essential regulatory labs and manufacturers may benefit from having several options available. Additionally, CDC shares data on U.S. seasonal flu viruses and performs analysis on viruses from other countries which informs future vaccine selection.
2. How might manufacturer decision-making be impacted by U.S. deviation from the WHO-led process to select seasonal flu vaccines?
The current process to select and produce seasonal flu vaccines relies on collaboration between WHO-GISRS, manufacturers, and national regulatory authorities.
- Would manufacturers be able to accommodate U.S. deviation from WHO recommendations? Just seven manufacturers are responsible for over 85% of global seasonal flu vaccine supply.[54] Manufacturers that supply multiple markets may be faced with the decision of whether to serve the U.S. market[55] over other markets (or vice versa). Additionally, U.S.-based vaccine manufacturers also supply vaccines outside the U.S.,[56] including quadrivalent vaccines targeting four seasonal flu strains (which differ from the trivalent vaccines used domestically).[57] Uncertainty in the U.S. strain selection process could introduce additional challenges for these manufacturers, potentially impeding production and supply for some.
- As detailed in the previous section, some manufacturers start producing certain flu vaccine components at risk in anticipation of WHO and FDA VRBPAC recommendations. Uncertainty about U.S. recommendations could introduce further risk into this equation, potentially resulting in unnecessarily wasted materials, production inefficiencies, or delays.
3. How would U.S. withdrawal from global flu surveillance and response impact the world’s ability to respond to seasonal flu?
- U.S. withdrawal from WHO/GISRS could result in less effective seasonal flu vaccines globally and for the U.S. Each year, tens of thousands of viral samples are shared with WHO flu collaborating centers.[58] As one of only five collaborating centers analyzing seasonal flu viruses, the U.S. CDC performs detailed analysis on thousands of samples each year which informs the seasonal flu vaccine selection.[59] The loss of this capacity may be detrimental to the ability to select optimal strains for seasonal flu vaccines. The former director of the flu collaborating center in Australia recently noted the large gap that would be left by the U.S. CDC and underscored the need for as much data as possible to inform vaccine composition decisions, stating that, “[i]f decisions are made with 30% less data, or 40% less data, that’s not good.”[60]
- U.S. withdrawal could weaken flu surveillance capacities in other countries. As discussed previously, CDC provides materials and other support to improve testing capacity in GISRS labs. A U.S. withdrawal could leave significant gaps, for example, if it no longer develops and shares updated diagnostic reagents to detect different flu viruses.
4. How would U.S. withdrawal from global flu surveillance and response impact the ability to respond to pandemic flu?
The 2017 HHS Pandemic Influenza Plan states that, “international activities serve to directly improve national security as they enable rapid communications, surveillance, and mitigation of emerging novel influenza viruses with other countries to ensure a better national response.”[61]
- U.S. withdrawal from global flu surveillance and response weakens both domestic and global capacity to prevent and respond to pandemics.
- WHO member states, including the U.S., share flu viruses with the potential to cause pandemics promptly, enabling rapid risk assessment and fast production of appropriate countermeasures to combat flu pandemics.[62]
- In preparation for potential pandemic flu, WHO vaccine composition meetings also assess and select viruses for vaccines for pandemic preparedness.[63] WHO flu collaborating centers, including the U.S. CDC, develop these candidate vaccine viruses and share them with other flu collaborating centers, essential regulatory labs, and manufacturers,[64] helping build stockpiles of key vaccine materials. Such stockpiles can shave months off of the timeline to produce vaccines deployed as a first line of defense against pandemic flu.[65] The U.S., for example, has a stockpile of pre-pandemic flu vaccine “building blocks” that, if well-matched to an emerging strain, can be filled into vials and deployed within weeks, with the potential to produce millions more doses over a few months.[66]
- Weakening GISRS could also limit the world’s ability to respond collectively to other threats. For example, the GISRS network contributed significantly to testing efforts during the COVID-19 pandemic, running 44.2 million tests for SARS-CoV-2 in 2020 and 2021.[67] This infrastructure bolsters response capabilities, helping to contain disease spread and protect people, including those in the U.S.
Conclusion
Several actions taken in the first month of the new Trump administration serve to cut the U.S. off from the rest of the world, diminish U.S. scientific and disease response capacity, and imperil U.S. global health programs and the people they help.
The global flu surveillance and response infrastructure underscores what is at stake when the U.S. disengages from WHO and broader global health cooperation. Weakening these systems within and among countries makes us all more vulnerable to outbreaks. The first Trump administration knew this. The 2017 National Security Strategy recognized that outbreaks impact national security “by taking lives, generating economic losses, and contributing to a loss of confidence in government institutions.” [68] To protect Americans, and people everywhere, the U.S. must fully engage in the work to detect and respond to disease threats.
References
[1] WHO media briefing on global health issues, at 17:04, https://www.youtube.com/watch?v=RGflJNNUR4E
[2]https://www.whitehouse.gov/presidential-actions/2025/01/withdrawing-the-united-states-from-the-worldhealth-organization/
[3]https://www.npr.org/sections/goats-and-soda/2025/01/29/nx-s1-5276340/trump-centers-for-disease-control-cdc-world-health-organization
[4]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[5]https://www.who.int/news-room/spotlight/history-of-vaccination/history-of-influenza-vaccination
[6] https://www.cdc.gov/orr/responses/h1n1-influenza-pandemic.html (accessed Feb. 23, 2025).
[7] https://www.nature.com/articles/s41541-023-00773-0
[8] https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal)
[9] https://www.cdc.gov/flu/about/index.html (accessed Feb. 24, 2025)
[10]https://web.archive.org/web/20250116010250/https://www.cdc.gov/flu/whats-new/flu-summary-addendum-2023-2024.html (archived link).
[11] https://www.cdc.gov/flu/about/index.html (accessed Feb. 24, 2025)
[12] https://www.who.int/initiatives/global-influenza-surveillance-and-response-system
[13]https://cdn.who.int/media/docs/default-source/vcm-southern-hemisphere-recommendation-2025/202409_qanda_recommendation_final.pdf?sfvrsn=bd3d90b1_3
[14] The WHO Pandemic Influenza Preparedness (PIP) Framework governs the sharing of potential pandemic flu viruses among WHO-GISRS members and with other entities, including manufacturers, and enables access to medical countermeasures to help combat pandemic flu. See, https://iris.who.int/bitstream/handle/10665/341850/9789240024854-eng.pdf?sequence=1
[15]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[16]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[17]https://www.who.int/docs/default-source/influenza/who-influenza-recommendations/vcm-southern-hemisphere-recommendation-2021/202009-qanda-recommendation.pdf
[18]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[19] https://www.stjude.org/research/global-impact/influenza-research-response.htm
[20]https://www.who.int/news-room/feature-stories/detail/celebrating-70-years-of-the-global-influenza-surveillance-and-response-system
[21] Id.
[22] For example, in 2014, a poor match between one of the strains in the seasonal flu vaccine and the strain that circulated resulted in 19% vaccine effectiveness in the U.S. Even without the mis-match that occurred during the 2014-15 flu season, seasonal flu vaccine effectiveness ranges between 49-60%. https://pmc.ncbi.nlm.nih.gov/articles/PMC5861780/
[23] https://wwwnc.cdc.gov/eid/article/28/13/21-2248_article; https://www.cdc.gov/flu/php/who-collaboration/index.html
[24] https://pmc.ncbi.nlm.nih.gov/articles/PMC4186468/
[25] https://pmc.ncbi.nlm.nih.gov/articles/PMC4186468/
[26] https://wwwnc.cdc.gov/eid/article/28/13/21-2248_article
[27]See, https://iris.who.int/bitstream/handle/10665/259400/WHO-WHE-IHM-GIP-2017.6-eng.pdf?sequence=1, at 7; https://iris.who.int/bitstream/handle/10665/44518/9789241548090_eng.pdf?sequence=1, at 15–6.
[28] https://archive.cdc.gov/www_cdc_gov/flu/spotlights/2018-2019/decade-since-h1n1-pandemic.html
[29] https://www.cidrap.umn.edu/influenza-general/cdc-contract-improve-labs-access-flu-viruses; https://www.internationalreagentresource.org/QuickLinks/Covid19FAQ.aspx#TOC11
[30] https://www.internationalreagentresource.org/QuickLinks/Covid19FAQ.aspx#TOC11; https://www.internationalreagentresource.org/International.aspx
[31] https://archive.cdc.gov/www_cdc_gov/flu/pdf/international/program/DIA-AnnualRept2016-2017.pdf
[32]https://pmc.ncbi.nlm.nih.gov/articles/PMC4947948/; https://www.fda.gov/consumers/consumer-updates/fdas-critical-role-ensuring-safe-and-effective-flu-vaccines; https://pmc.ncbi.nlm.nih.gov/articles/PMC2843114/
[33]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[34]https://cdn.who.int/media/docs/default-source/influenza/national-influenza-centers-files/nic_tor_en.pdf?sfvrsn=93513e78_30
[35]https://www.who.int/news-room/feature-stories/detail/seventy-years-of-gisrs—the-global-influenza-surveillance—response-system
[36]https://www.who.int/news-room/events/detail/2025/02/24/default-calendar/who-consultation-on-the-composition-of-influenza-virus-vaccines-for-use-in-the-2025-2026-northern-hemisphere-influenza-season; https://www.who.int/news-room/events/detail/2025/02/28/default-calendar/who-information-meeting-on-the-composition-of-influenza-virus-vaccines-for-use-in-the-2025-2026-northern-hemisphere-influenza-season
[37] https://pmc.ncbi.nlm.nih.gov/articles/PMC4947948/
[38] Id.
[39] Id.
[40] https://www.fda.gov/media/137990/download, at 147.
[41] These institutions also provide such materials needed for the production of vaccines for pandemic preparedness purposes.
[42] CVVs should grow well in either eggs or cells and should be determined by WHO flu CCs to be antigenically similar to the virus that has been recommended for use in vaccines—necessary parts of ensuring viruses can be used for the timely production of effective vaccines. See, https://cdn.who.int/media/docs/default-source/influenza/who-influenza-recommendations/vcm-northern-hemisphere-recommendation-2024-2025/202402_frequently-asked-questions.pdf?sfvrsn=88eb9509_4
[43] https://www.fda.gov/vaccines-blood-biologics/science-research-biologics/cbers-research-scientists (accessed Feb. 16, 2025)
[44] https://pmc.ncbi.nlm.nih.gov/articles/PMC4947948/
[45] Id.
[46] https://www.statnews.com/2025/02/13/who-flu-vaccine-strain-selection/; https://insights.citeline.com/pink-sheet/product-reviews/us-advisory-committees/us-fda-advisory-committee-freeze-raises-concerns-of-delayed-more-controversial-approvals-CWT2HOAQ3JBHNCMKSSOOXVAYYU/
[47] https://www.fda.gov/advisory-committees/advisory-committee-calendar (accessed Feb. 25, 2025)
[48] In 2019, WHO delayed its recommendation for one component of the vaccine by one month in order to incorporate additional data. This elicited warnings from manufacturers that this would likely cause delays to market supply. See, https://cdn.who.int/media/docs/default-source/influenza/who-influenza-recommendations/vcm-northern-hemisphere-recommendation-2019-2020/201902-qanda-recommendation-ah3n2.pdf?sfvrsn=634ba5d4_7; https://www.ifpma.org/news/statement-on-influenza-vaccine-supply-in-the-2019-20-northern-hemisphere-season/
[49] Seasonal Influenza Vaccine Supply for the U.S. 2024-2025 Influenza Season, https://archive.cdc.gov/www_cdc_gov/flu/prevent/vaxsupply.htm
[50]https://www.cdc.gov/acip-recs/hcp/vaccine-specific/flu.html; https://www.cdc.gov/mmwr/volumes/73/rr/rr7305a1.htm (accessed Feb. 25, 2025)
[51] https://www.cdc.gov/acip/meetings/index.html (accessed Feb. 25, 2025)
[52] WHO includes a list of available CVVs determined to be antigenically similar to the recommended vaccine viruses. See, https://cdn.who.int/media/docs/default-source/influenza/who-influenza-recommendations/vcm-northern-hemisphere-recommendation-2024-2025/202402_frequently-asked-questions.pdf (answering the question “What does the term “-like virus” mean in the vaccine composition recommendation?”).
[53] See e.g., https://cdn.who.int/media/docs/default-source/influenza/cvvs/cvv-northern-hemisphere-2024-2025/summary_a_h1n1_cvv-egg_nh24-25.pdf?sfvrsn=5609fa26_6 (showing WHO’s recommendations for influenza A(H1N1)pdm09 egg-derived candidate vaccine viruses and available reference reagents for the 2024-2025 northern hemisphere influenza season).
[54]https://cdn.who.int/media/docs/default-source/immunization/mi4a/who_mi4a_global_market_study_seasonal_influenza_vaccine.pdf?sfvrsn=9f24acbf_3&download=true
[55] This flu season, the U.S. expects to receive about 148 million doses of flu vaccines. See,https://www.cdc.gov/fluvaxview/dashboard/index.html (accessed Feb. 23, 2025).
[56] For example, two U.S. vaccine manufacturers have been approved to produce Southern Hemisphere formulations of their flu vaccine (Sanofi Fluzone and Seqirus Afluria). See, https://www.fda.gov/media/182604/download
[57] As of the 2024-2025 flu season in the U.S., all available flu vaccines are trivalent (targeting an influenza A(H1N1) virus, an influenza A(H3N2) virus, and an influenza B/Victoria lineage virus). Previously, U.S. flu vaccines were quadrivalent (targeting those viruses previously mentioned, plus a B/Yamagata lineage virus). In September 2023, WHO recommended that the B/Yamagata component be removed from flu vaccines because the GISRS network had not detected it in over three years—indicating that it is unlikely to be circulating in the population and thus, no longer necessary in vaccines. Following this recommendation, this change was implemented in the U.S. However, both WHO and VRBPAC continue to include recommendations for quadrivalent vaccines for countries that have not yet implemented this change (owing to differing capacities and regulatory architecture between countries). See, https://cdn.who.int/media/docs/default-source/influenza/who-influenza-recommendations/vcm-southern-hemisphere-recommendation-2024/202309_recommendation.pdf?sfvrsn=2c2cbebd_8&download=true (detailing WHO recommendation to remove B/Yamagata); https://www.cdc.gov/flu/vaccine-types/trivalent.html (noting trivalent composition vaccines distributed in the U.S.) (accessed Feb. 16, 2025).
[58]https://www.who.int/news-room/feature-stories/detail/celebrating-70-years-of-the-global-influenza-surveillance-and-response-system
[59] https://cdcmuseum.org/exhibits/show/influenza/scientific-breakthroughs-giss/surveillance-vaccines
[60] https://www.statnews.com/2025/02/13/who-flu-vaccine-strain-selection/
[61] https://www.cdc.gov/pandemic-flu/media/pan-flu-report-2017v2.pdf
[62] Similar to seasonal flu viruses, CDC plays a major role in GISRS receiving and analyzing potential pandemic flu viruses. CDC’s absence could mean less capacity to perform this analysis globally.
[63]https://www.who.int/news-room/events/detail/2025/02/24/default-calendar/who-consultation-on-the-composition-of-influenza-virus-vaccines-for-use-in-the-2025-2026-northern-hemisphere-influenza-season
[64] https://www.cdc.gov/bird-flu/php/severe-potential/candidate-vaccine-virus.html
[65] https://www.cdc.gov/bird-flu/php/severe-potential/candidate-vaccine-virus.html; https://medicalcountermeasures.gov/barda/influenza-and-emerging-infectious-diseases/pandemic-vaccines-adjuvants/
[66] https://aspr.hhs.gov/H5N1/Pages/default.aspx
[67]https://www.who.int/news-room/feature-stories/detail/celebrating-70-years-of-the-global-influenza-surveillance-and-response-system
[68] https://trumpwhitehouse.archives.gov/wp-content/uploads/2017/12/NSS-Final-12-18-2017-0905.pdf