How Inadequate Supply Drives Inequities in Global COVID-19 Access
Rich Country Vaccine Hoarding, Lack of Tech-Transfer, and Failing to Rapidly Scale Manufacturing Are Driving Global Vaccine Apartheid
How Inadequate Supply Drives Inequities in Global COVID-19 Access (pdf)
Contents
THERE IS A VACCINE SHORTAGE IN AFRICA.
AFRICAN VACCINE HESITANCY IS SIMILAR TO THAT IN RICH COUNTRIES.
INADEQUATE SUPPLY PREVENTS CONSTRUCTION OF DISTRIBUTION SYSTEMS AND PUBLIC HEALTH EDUCATION.
OMICRON LIKELY WILL EXACERBATE SUPPLY SHORTAGES.
HISTORY WARNS AGAINST BLAMING AFRICANS.
VACCINE APARTHEID
The Omicron variant is focusing renewed attention on vaccine apartheid – the sharp divergence in vaccine availability and vaccination rates in rich and poor countries. There has been some closing of the vaccine gap in the last six months, but the divergence remains especially sharp between rich nations and countries in Africa. Overall, the vaccination rate in rich countries is six times higher than the rate in African nations.
Vaccine apartheid is a tremendous moral and humanitarian failing by the international community. It has left people in poorer nations needlessly subject to illness and death and had ongoing, devastating effects on global poverty; Covid has caused an “historically unprecedented” increase in global poverty, with the worst ongoing effects in Africa.
Vaccine apartheid is also having boomerang effects on rich countries. The economic slowdown in poor countries is impacting rich nations, as well. And, most consequentially, permitting the pandemic to rage in poorer countries increases the risk of new variants emerging.
With renewed focus on vaccine apartheid, there are suggestions that the issue is no longer about ensuring adequate vaccine supply, but only about overcoming vaccine hesitancy and distribution challenges. This argument is wrong, or at least incomplete. In fact, there have not been and are not enough vaccines available to African countries. And, while hesitancy and distribution are real problems, they are not unrelated to supply constraints.
THERE IS A VACCINE SHORTAGE IN AFRICA
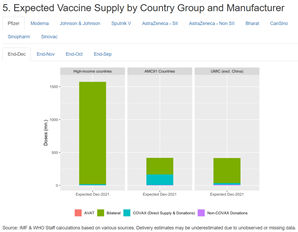
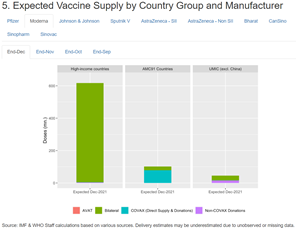
Global vaccine manufacturing supply has consistently run far behind projections; the United States and other rich country governments have failed to take measures to share vaccine technology and expand production; and rich countries have consistently hoarded the supplies that exist. With no technology sharing, poorer nations are dependent on donations, which also have run behind projections. As a result of this combination of factors, there is an objective shortfall of available vaccines in poor countries, especially African nations.
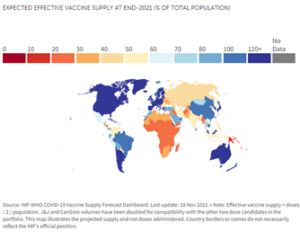
The International Monetary Fund and World Health Organization project that, by the end of this year, available supply in 73 countries will be inadequate to meet 40 percent of population target – itself, very inadequate.
Pfizer and Moderna especially have focused on providing doses to high-income countries, which have received the overwhelming majority of doses manufactured by the two corporations to date.
More people have received a booster shot in the United States than have received a first dose in eight Southern African countries combined. People in Botswana are traveling to other countries in order to get vaccinated.
AFRICAN VACCINE HESITANCY IS SIMILAR TO THAT IN RICH COUNTRIES
It is true that there is worrisome evidence of vaccine hesitancy in African countries and around the world. But overall vaccine hesitancy appears to be less in Africa than in the United States and some other rich nations. A survey conducted by the Africa Centres for Disease Control and Prevention (Africa CDC), in partnership with the London School of Hygiene & Tropical Medicine (LSHTM) has shown that a predominant majority (79% average) of respondents in Africa would take a COVID-19 vaccine if it were deemed safe and effective. By contrast, about 73 percent of Americans say they have been vaccinated or plan to be – the second lowest rate among rich nations.
To make this plain: While hesitancy is a comparable or slightly worse problem in the United States, the U.S. vaccination rate is six times higher than for Africa overall.
The Africa CDC results on hesitancy are consistent with other surveys on hesitancy in low- and middle-income countries. A Nature review of 15 studies finds “considerably higher willingness to take a COVID-19 vaccine” in low- and middle-income countries than in the United States.
INADEQUATE SUPPLY PREVENTS CONSTRUCTION OF DISTRIBUTION SYSTEMS AND PUBLIC HEALTH EDUCATION
Although hesitancy rates may be lower in African countries than in the United States, it is a problem. And of course African public health systems are weak and underfunded and face challenges in distributing vaccines, including those that require cold storage, or as is uniquely the case with the Pfizer-BioNTech vaccine, ultracold storage.
However, it is important to understand that these problems are exacerbated by supply shortages. Simply put, countries cannot reasonably undertake public health education programs promoting Covid vaccination if they cannot actually make vaccines available to the public. And they can’t reasonably invest in distribution systems if they don’t have vaccines to fill a distribution pipeline, or if vaccine supplies are delivered erratically and near expiration.
As a joint statement from the African Union, African CDC, World Health Organization and others explains, “[T]he majority of the donations to-date have been ad hoc, provided with little notice and short shelf lives. This has made it extremely challenging for countries to plan vaccination campaigns and increase absorptive capacity.”
The joint statement elaborates:
“Countries need predictable and reliable supply. Having to plan at short notice and ensure uptake of doses with short shelf lives exponentially magnifies the logistical burden on health systems that are already stretched. Furthermore, ad hoc supply of this kind utilises capacity – human resources, infrastructure, cold chain – that could be directed towards long-term successful and sustainable rollout. It also dramatically increases the risks of expiry once doses with already short shelf-lives arrive in country, which may have long-term repercussions for vaccine confidence.”
OMICRON LIKELY WILL EXACERBATE SUPPLY SHORTAGES
Early evidence suggests that boosters of the mRNA vaccines may provide meaningful protection against the Omicron variant. Increased demand for boosters in rich and upper-middle income countries will diminish supply available for poorer nations – while increasing the volume need in those same countries.
It is too early to know at all what kind of protection the non-mRNA vaccines may provide against Omicron. If boosters are needed, there will be dramatically increased need in poorer countries, beyond existing manufacturing capacity. If those vaccines offer inadequate protection, even when boosted, and the world becomes more reliant on mRNA vaccines, then the supply shortage will be even more stark.
Airfinity predicts that if a new vaccine is needed for Omicron, the world could produce 6 billion doses by the end of 2022. Absent a radical shift in how vaccines have been allocated, that scenario would almost certainly mean very few vaccines made available for poorer countries. We could see the next phase of vaccine apartheid.
HISTORY WARNS AGAINST BLAMING AFRICANS
In 2001, the director of the U.S. Agency for International Development, Andrew Natsios, said that Africans “don’t know what Western time is,” and therefore could not manage complicated regimens for HIV/AIDS drugs. Others, more sophisticated, more knowledgeable and better intentioned, warned about Africa’s lack of “absorptive capacity” for HIV/AIDS drugs.
But the catastrophic delay in making treatments available for HIV/AIDS turned out to be a problem, first and foremost of affordable supply. There were hard challenges to be overcome in terms of distribution and provision of care. But when AIDS drugs became affordable and available, those challenges were, in large part, met (including the with major assistance from the U.S. PEPFAR program and other international support).
The lessons to be learned from this experience are: 1) there can be no widespread treatment (or vaccination) without adequate supply; and 2) while public health infrastructure is absolutely inadequate in many African nations, provision of adequate supply of vital medicines (or vaccines) can be catalytic in driving solutions to those problems. We must not repeat the mistake of citing Africa’s public health deficiencies as a rationalization or excuse for global failures to make available vital medicines or vaccines.